UNDERSTANDING EFFECT OF HIGH PROLACTIN IN MEN

High prolactin levels in men can interfere with the hormones responsible for reproduction. Elevated prolactin may reduce the release of gonadotropin-releasing hormone (GnRH), which in turn lowers luteinizing hormone (LH), follicle-stimulating hormone (FSH), and testosterone levels. This hormonal imbalance can affect sperm production, including sperm count, motility, and morphology. However, not all men with high prolactin experience problems with sperm production or fertility. In many cases, the more common effects are low libido and erectile dysfunction. It is also important to note that not every man with low libido requires medication to lower prolactin levels. Some men may benefit from lifestyle changes such as improving their diet, reducing stress, getting adequate rest, and taking supplements that support relaxation and overall well-being. These changes can help improve libido naturally. Top of Form Bottom of Form
HYDROCOELE AND VARICOCELE IN MALE INFERTILITY
Hydrocele and varicocele are conditions that can affect male fertility by reducing sperm function, sperm quality, and sperm count. A hydrocele occurs when fluid builds up in the sac surrounding the testicle, causing swelling and a feeling of heaviness in the scrotum. It is usually visible and may cause discomfort or pain. A varicocele occurs when the veins inside the scrotum become enlarged or dilated, similar to varicose veins. Varicoceles are graded based on severity and may not be noticeable in the early stages. In advanced cases, they can become visible or more painful. One common symptom of both conditions is pain or discomfort in the testicles. They can also contribute to low sperm count, poor sperm motility, and abnormal sperm morphology, which may affect fertility. Anyone experiencing symptoms of hydrocele or varicocele should consult a qualified healthcare professional for proper diagnosis and treatment.
FIBROID MAY AFFECT YOUR FALLOPIAN TUBES NEGATIVELY
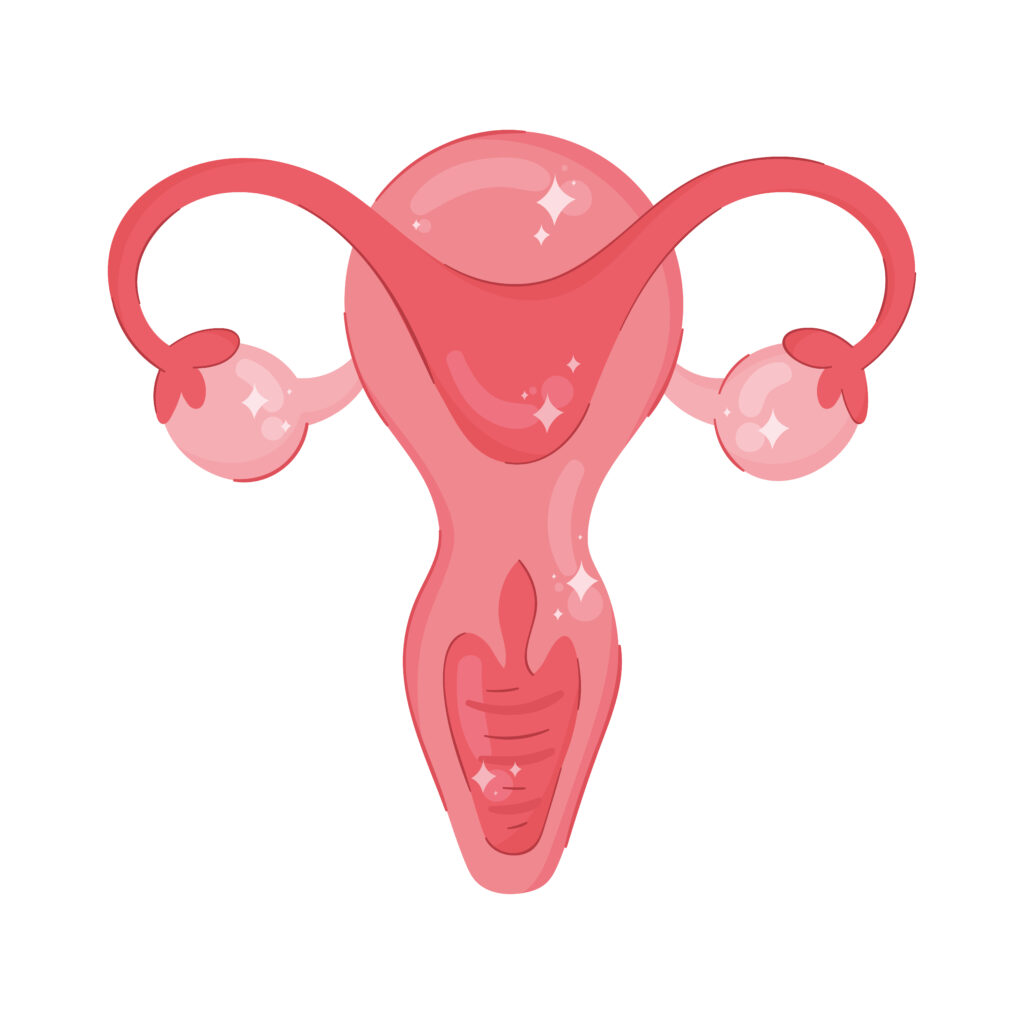
Fibroids do not always prevent pregnancy, especially when they are located outside the uterus. However, their size and location can still affect fertility in some women. Even if a fibroid is not inside the womb, it may put pressure on nearby structures such as the fallopian tubes. In some cases, this pressure can interfere with the normal function of the tubes or contribute to blockage over time, which may make it more difficult to conceive. Every case is different, and not all fibroids cause fertility problems. That is why proper medical evaluation is important. If you have fibroids and are trying to get pregnant, it is advisable to consult a qualified healthcare professional for assessment and appropriate treatment options.
EVACUATION YOU DID TO REMOVE PREGNANCY COULD BE THE CAUSE OF YOUR INFERTILITY

Evacuation is a procedure used to remove a pregnancy from the womb (uterus). In medical terms, it is called Dilation and Curettage (D&C). During early pregnancy, the embryo attaches firmly to the lining of the uterus, known as the endometrium. This lining is very important because it allows the pregnancy to implant and grow properly. In a D&C procedure: The cervix is gently opened (dilation). A medical instrument is used to remove pregnancy tissue from the uterus (curettage). When this procedure is done by a qualified professional using proper techniques (often with ultrasound guidance), it is generally safe. However, if it is done improperly or by an untrained person, it can damage the lining of the uterus. Possible complications include: Scratching or scarring of the endometrium Thinning of the uterine lining Formation of scar tissue inside the uterus (adhesions) These scars may not affect your monthly menstrual cycle, but they can make it difficult for a future pregnancy to implant properly, which may lead to infertility or repeated miscarriages. If you have concerns about infertility after a D&C, it is important to see a qualified healthcare professional for proper evaluation and guidance
EVACUATION YOU DID TO REMOVE PREGNANCY COULD BE THE CAUSE OF YOUR INFERTILITY

Evacuation is a procedure used to remove a pregnancy from the womb (uterus). In medical terms, it is called Dilation and Curettage (D&C). During early pregnancy, the embryo attaches firmly to the lining of the uterus, known as the endometrium. This lining is very important because it allows the pregnancy to implant and grow properly. In a D&C procedure: The cervix is gently opened (dilation). A medical instrument is used to remove pregnancy tissue from the uterus (curettage). When this procedure is done by a qualified professional using proper techniques (often with ultrasound guidance), it is generally safe. However, if it is done improperly or by an untrained person, it can damage the lining of the uterus. Possible complications include: Scratching or scarring of the endometrium Thinning of the uterine lining Formation of scar tissue inside the uterus (adhesions) These scars may not affect your monthly menstrual cycle, but they can make it difficult for a future pregnancy to implant properly, which may lead to infertility or repeated miscarriages. If you have concerns about infertility after a D&C, it is important to see a qualified healthcare professional for proper evaluation and guidance
HOW TO HANDLE A WOMAN WITH A LOW SEX DRIVE

Low sexual desire (low libido) in women can sometimes be caused by hormonal imbalance. In some cases, this imbalance may begin as early as puberty and continue into adulthood, affecting sexual desire and responsiveness. Hormones such as estrogen, progesterone, and testosterone play important roles in a woman’s sexual drive. When these hormones are not balanced, it can reduce interest in sex, cause vaginal dryness, or make arousal more difficult. If a woman experiences persistent low libido, she should see a qualified healthcare professional for proper evaluation and treatment. Hormonal testing, counseling, or other medical support may help address the issue. The Partner’s Role A supportive partner also plays an important role. Communication is key: Informing your partner ahead of time about your desire for intimacy can help her prepare emotionally and mentally. Emotional readiness often influences physical readiness. Avoid rushing: Instead of immediate penetration, begin with affectionate touch and foreplay. This helps stimulate arousal, increase natural lubrication, and align both partners emotionally and physically. Patience, understanding, and open communication can greatly improve intimacy and sexual satisfaction for both partners.
HOW MUCH DO YOU KNOW ABOUT PCOS

Many people think that if a woman has regular monthly periods, she cannot have Polycystic Ovary Syndrome (PCOS). That is not always true. PCOS is a hormonal condition that affects how the ovaries function. While irregular periods are common with PCOS, some women still have what appears to be a normal menstrual cycle. However, they may still have other underlying hormonal imbalances affecting ovulation and fertility. In some cases, a woman may notice that: Her periods are usually regular But once she starts fertility treatment or hormonal medications, her cycle becomes irregular She may experience delayed ovulation or no ovulation at all This could reveal an underlying hormonal issue such as PCOS that was not previously obvious. Why This Happens PCOS is mainly related to: Hormonal imbalance (especially excess androgens) Insulin resistance Problems with regular ovulation Even if bleeding occurs every month, ovulation may not be happening properly. This is called anovulatory cycles, and it can affect fertility. What You Should Do If you notice changes in your cycle during fertility treatment, or if you are struggling to conceive despite having regular periods, it is important to: See a qualified healthcare professional Do hormonal testing Get a pelvic ultrasound scan Properly evaluate whether it is simple hormonal imbalance or PCOS Early diagnosis helps guide the right treatment and improves chances of successful conception.
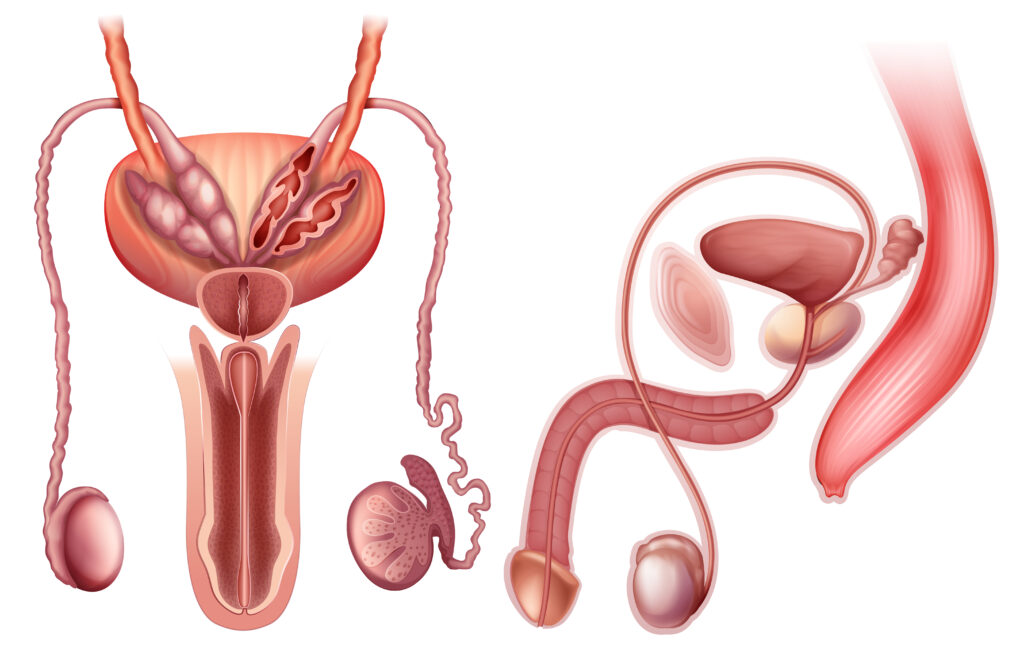
UNEXPLAINED INFERTILITY: LOW SPERM VOLUME IN MEN

Low sperm volume (low semen volume) is an important but often overlooked cause of infertility. Many couples focus only on the woman’s health, but male factors contribute to infertility in a significant number of cases. What Is Ejaculation? Ejaculation happens when a man reaches orgasm and releases semen from the penis into the vagina. Semen is the fluid that contains: Sperm cells (which fertilize the egg) Fluids from the prostate and seminal vesicles Normally, semen volume ranges from about 1.5 to 5 milliliters per ejaculation. When the volume is very low, it may reduce the chances of pregnancy because fewer sperm are delivered into the female reproductive tract. Why Low Sperm Volume Matters Low sperm volume can: Reduce the number of sperms reaching the egg Make fertilization more difficult Indicate a blockage in the reproductive tract Suggest hormonal imbalance or gland problems Even if sperm cells are healthy, very low semen volume can affect the ability to conceive. Possible Causes of Low Sperm Volume Frequent ejaculation (not allowing enough time for semen to build up) Hormonal imbalance Blockage of the vas deferens (the tube that carries sperm) Problems with the seminal vesicles or prostate gland Retrograde ejaculation (where semen flows backward into the bladder) Dehydration or certain medications The Role of the Vas Deferens The vas deferens is the tube that carries sperm from the epididymis (where sperm mature at the back of the testicle) to mix with seminal fluid before ejaculation. If this tube is blocked or damaged: Semen volume may be low Sperm may be absent (azoospermia) Fertility may be affected Semen Analysis and Abstinence For accurate semen analysis, most medical guidelines recommend abstaining from ejaculation for 2–7 days before the test. This helps standardize the result and provides a clearer picture of sperm count, motility, and volume. Testing too soon after ejaculation may temporarily reduce volume and sperm count, which can give misleading results. Therefore, it is important to follow proper medical guidelines rather than personal opinion when preparing for a semen test. Important Clarification for Couples While women may not always clearly notice ejaculation, pregnancy does not depend on sensation alone. What matters most is: Adequate semen volume Healthy sperm count Good sperm motility (movement) Proper timing during ovulation When to See a Doctor A man should seek evaluation if: Pregnancy has not occurred after 12 months of regular unprotected intercourse There is very little or no semen during ejaculation There are known testicular, hormonal, or sexual health issues A fertility specialist can perform proper testing and determine the exact cause.
10 THINGS YOU NEED TO KNOW ABOUT SURROGACY

1. Gestational Surrogacy In gestational surrogacy, the surrogate carries a pregnancy but does not use her own egg. The embryo is created through In Vitro Fertilization (IVF) using: The intended mother’s egg and intended father’s sperm, or Donor egg and/or donor sperm The embryo is then transferred into the surrogate’s uterus. In this case, the surrogate has no genetic connection to the baby. She is only carrying the pregnancy. This type of surrogacy: Requires IVF Requires strong legal agreements Is the most commonly practiced form today 2.Traditional Surrogacy In traditional surrogacy, the surrogate uses her own egg, meaning she is genetically related to the baby. Her egg is fertilized with the intended father’s sperm (usually through artificial insemination). Because the surrogate is the biological mother, this type carries more legal and emotional complexity and is less commonly practiced in many countries. Important Facts About Surrogacy Surrogacy Is Not the Same as Adoption Adoption is a legal process where a person or couple becomes the legal parent(s) of a child who is not biologically theirs. In gestational surrogacy, the child is usually genetically related to the intended parents. The surrogate is simply carrying the pregnancy. IVF Is Required (in Gestational Surrogacy) Gestational surrogacy requires IVF to create and transfer the embryo into the surrogate’s uterus.The Surrogate Does Not Always Donate Her Eggs In gestational surrogacy, only the womb is needed — not the surrogate’s egg. In traditional surrogacy, her egg is used. It Involves Intended Parents While surrogacy often involves a married couple, laws in some countries also allow single individuals or unmarried couples to pursue surrogacy. Legal eligibility depends on the country’s regulations. Legal Documentation Is Essential Surrogacy must involve proper legal agreements to: Define parental rights Protect the surrogate Protect the intended parents Prevent future disputes Without legal documentation, serious complications can arise. Screening Is Mandatory Before proceeding, the surrogate should undergo: Medical and fertility screening Psychological evaluation Mental health assessment Infectious disease testing This ensures she is physically and emotionally prepared for the process. It Is Expensive Surrogacy can be costly due to: IVF procedures Medical care Legal fees Compensation (where allowed) Agency fee It Is Illegal in Some Countries Surrogacy laws vary widely. Some countries: Fully allow it Restrict it Completely prohibit it It is important to understand the laws in your country before starting the process It Is Not 100% Guaranteed Like all fertility treatments, surrogacy does not guarantee pregnancy or a successful birth. Success depends on: Egg and sperm quality Uterine health Age Overall medical factors Multiple attempts may sometimes be required. Emotional Commitment Is Important Surrogacy is not just a medical process — it is emotional for everyone involved. Clear communication, counseling, and support are crucial throughout the journey.
WHEN YOUR MENSTRUAL PERIOD IS PAINFUL IT COULD BE A SERIOUS SIGN OF INFERTILITY

I want to discuss a painful menstruation in relation to adenomyosis and endometriosis. Normally, menstrual cycle supposed not to come with pain and if there will me any, it should be a mild one not a severed one. The duration as designed by God should be between two to seven days. When you start having a sever pain or heavy menstrual flow, it may be that you are suffering from endometriosis or adenomyosis but endometriosis is a bit mild, it is usually caused when the inner tissue that serves as a as lining in the endometrium in the area of the womb, start shedding blood, the other part of the womb that has the tissue will want to shed blood as well causing you to have a severe pain and it can be surgically removed by the professionals and can also be managed. In the cause of the adenomyosis, is when the blood flows into itself, and prevent women from getting pregnant. in this case, if it can’t be managed, it may lead to the removal of the womb. What you need to do is to visit the professional on what to do and stay away from self-medication which may escalate the issue to the point of infertility.