WHEN YOU FEEL AS IF SOMETHING IS BREATHING OR LOCALIZED PAIN AROUND YOUR OVARIES

Some women experience a strange sensation around the waist or lower back during their cycle. While this feeling can be caused by many harmless reasons—such as muscle tension, hormonal changes, or nerve sensitivity—it is not a proven sign of having many immature eggs or of developing follicular cysts/PCOS. Polycystic Ovary Syndrome (PCOS) has specific symptoms such as irregular periods, acne, excessive hair growth, weight changes, and difficulty ovulating. It cannot be diagnosed based on sensations alone. If you are experiencing unusual or persistent sensations—especially while taking fertility-related medication—you should not stop the medication on your own. Instead, consult a healthcare professional for proper evaluation, hormone tests, or an ultrasound to determine the actual cause and the right treatment.
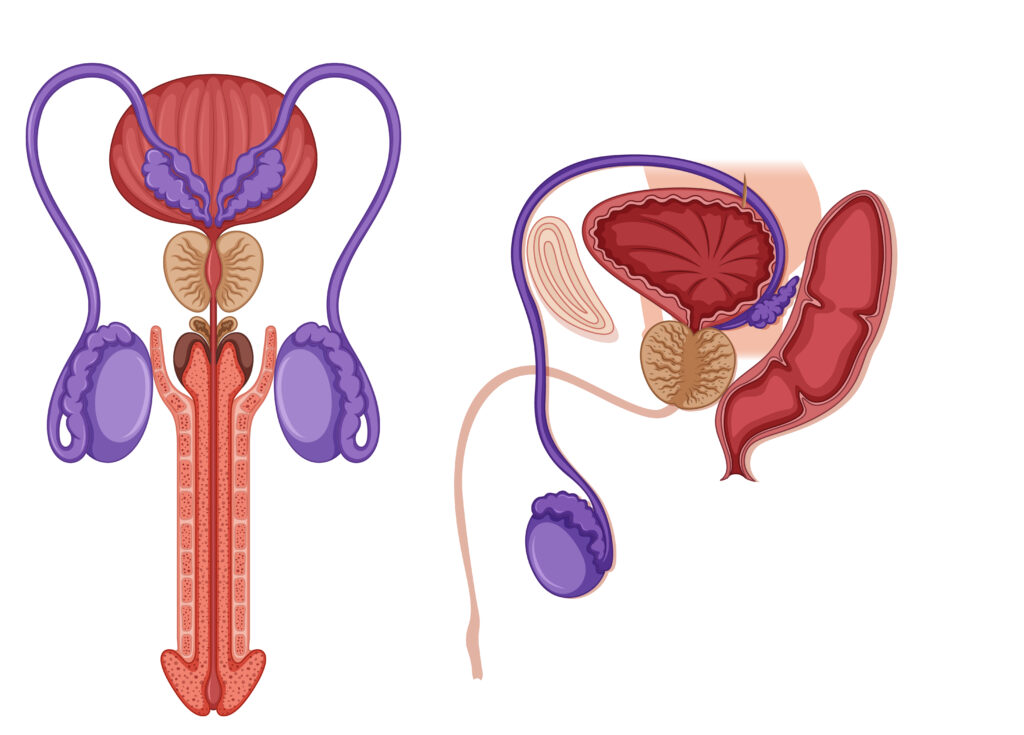
FAILED IVF: WHEN SEMEN QUALITY IS CLAIMED TO BE THE CAUSE
When IVF fails and the issue appears to be sperm-related, patients often ask why the clinic did not cancel the procedure if the sperm was “not good enough.” It is important to understand that semen analysis and sperm function tests are different. A semen analysis only measures sperm count, motility, morphology, and pH. It is not a fertility test; rather, it assesses the testicles’ ability to produce sperm of reasonable quality. However, it cannot reliably determine a sperm cell’s fertilization potential. Patients sometimes ask why they are not sent for a sperm function test instead. The reason is that not all centres have the technology to perform sperm function tests. In many cases, we only discover problems with sperm fertilization ability when we observe poor embryo development after IVF, despite having a good egg and an apparently normal semen analysis. For a sperm cell to fertilize an egg—whether naturally, through IUI, or through IVF—it must successfully complete five key processes: 1. Capacitation – occurs inside the female reproductive tract; it cannot be evaluated directly. 2. Acrosome Reaction – the sperm’s ability to bind to the egg’s outer layer; this requires advanced technology to assess. 3. Zona Pellucida Binding – when enzymes in the sperm head are released, allowing it to penetrate the egg. 4. Nuclear Decondensation – the genetic material of the egg and sperm combine to form a fertilized ovum. 5. (Implied final step) Successful formation of a healthy embryo. Because semen analysis cannot evaluate these functional steps, a sperm sample may appear normal yet still fail to fertilize an egg.
FOLIC ACID IS NOT A FERTILITY SUPPLEMENT
Folic acid is one of the most common medications taken by women hoping to conceive, but it is not a fertility supplement. Its main role is to support red blood cell formation in the mother and to help prevent brain and spinal cord defects in the baby. Women who are trying to conceive should understand that folic acid alone does not correct hormonal problems, trigger ovulation, improve overall fertility, or unblock fallopian tubes. It is important to consult a professional and undergo the appropriate tests—such as AMH, FSH, LH, progesterone, and estradiol—so that the right treatment plan can be created for you. Folic acid can then be added as part of your overall pre-conception care.
OBESITY COULD AFFECTS FERTILITY NEGATIVELY

Obesity can occur in two primary forms. The first type results from lifestyle factors—particularly overeating and having the financial means to consume whatever food one desires, often leading to a high intake of processed or calorie-dense foods. The second type of obesity is more complex and may occur naturally in some individuals due to genetic or metabolic factors, even if they do not eat excessively. This type is often influenced by hereditary traits, hormonal imbalances, or underlying medical conditions. The purpose of this write-up is to highlight how obesity can negatively affect fertility, particularly in women. Obesity is closely linked to hormonal imbalances. Excess fat tissue in the body can lead to increased production of insulin—a hormone that helps regulate blood sugar. When the body produces too much insulin, it can lead to a condition called insulin resistance, where the cells become less responsive to insulin. This condition causes the body to produce even more insulin to compensate. High insulin levels can increase the production of androgens (male hormones like testosterone) in a woman’s body. Additionally, fat cells can convert androgens into estrogen, further disrupting the hormonal balance. These hormonal shifts interfere with the normal functioning of the ovaries, particularly the development and release of eggs (ovulation). As a result, women with obesity may experience irregular menstrual cycles, difficulty ovulating, or even complete absence of ovulation (anovulation), all of which contribute to infertility. Elevated androgen levels also impair the development of ovarian follicles—the small sacs in the ovaries where eggs grow—making conception more difficult.
5 MAJOR CAUSES OF IVF FAILURE.
Embryo transfer is a critical step in the In Vitro Fertilization (IVF) process. Even when good-quality embryos are used, some transfers still fail. Below are five major causes of such failures, along with explanations and solutions. Uterine Issues The uterus (womb) must be in optimal condition for an embryo to successfully implant. Several problems within the uterus can prevent this: Polyps: These are small growths inside the uterine lining that can interfere with implantation. Adhesions (Asherman’s Syndrome): Scar tissue inside the uterus, usually from past surgeries or infections, can block implantation. Fibroids: These are non-cancerous growths. If they are within or near the uterine cavity, they can distort it and reduce success rates. Ulterine cavity abnormalities A uterus that is not “free” or open (e.g., narrow cavity) cannot support embryo implantation properly. Doctors often recommend a hysteroscopy before starting IVF. This procedure allows them to see inside the uterus and remove any obstacles (polyps, fibroids, scar tissue, etc.) that may hinder implantation. Hydrosalpinx This refers to a condition where the fallopian tubes are swollen and filled with fluid, often due to previous infections (like pelvic inflammatory disease). The fimbriae (finger-like ends of the fallopian tubes) become blocked. The fluid from the tubes can leak into the uterus and harm the embryos, making implantation unlikely. Hydrosalpinx must be treated before IVF begins. Often, the fallopian tubes are removed (salpingectomy) or blocked off to prevent the toxic fluid from reaching the uterus. Inadequate Fertility Treatment (Hormonal Imbalance) Hormones must be in the right balance for IVF to work. Key hormones include: LH (Luteinizing Hormone) FSH (Follicle-Stimulating Hormone) AMH (Anti-Müllerian Hormone) – an indicator of ovarian reserve If any of these are out of range, the body may not respond well to fertility medication, resulting in poor egg quality or uterine lining problems. Get your hormone levels tested before treatment. If there’s an imbalance, your doctor may recommend hormone therapy or other medications for 1-2 months to stabilize your system before IVF. Poor Embryo Quality Even if everything is perfect in the uterus, if the embryo itself is not healthy, implantation will likely fail. Embryos are graded (e.g., Grade A, B) based on how they look under a microscope. The developmental stage also matters Blastocyst (Day 5 embryo) is usually preferred over earlier stages (e.g., morula). Poorly graded embryos have lower chances of implantation and pregnancy. Ask about the quality and grade of the embryo being transferred. Consider genetic testing (PGT-A) if you’ve had repeated failures, to check for chromosomal abnormalities Difficulty During Embryo Transfer Procedure Even if the embryo is good and the uterus is healthy, technical issues during the transfer can cause failure: Cervical stenosis: Narrow or tight cervix that makes it hard to insert the catheter. Uterine angle or position: May make the passage of the catheter difficult. Bloody transfer: If the catheter causes trauma and bleeding during the procedure, blood can be toxic to the embryo. Vaginal stenosis: Narrowing of the vaginal canal, possibly from past procedures or radiation therapy, can complicate the transfer. A sono-hysterogram or mock transfer may be done in advance to check if the cervix is easy to pass. If stenosis is detected, cervical dilatation may be done beforehand. Ensure a skilled clinician is performing the embryo transfer with utmost precision.
ENDOMETRIOSIS
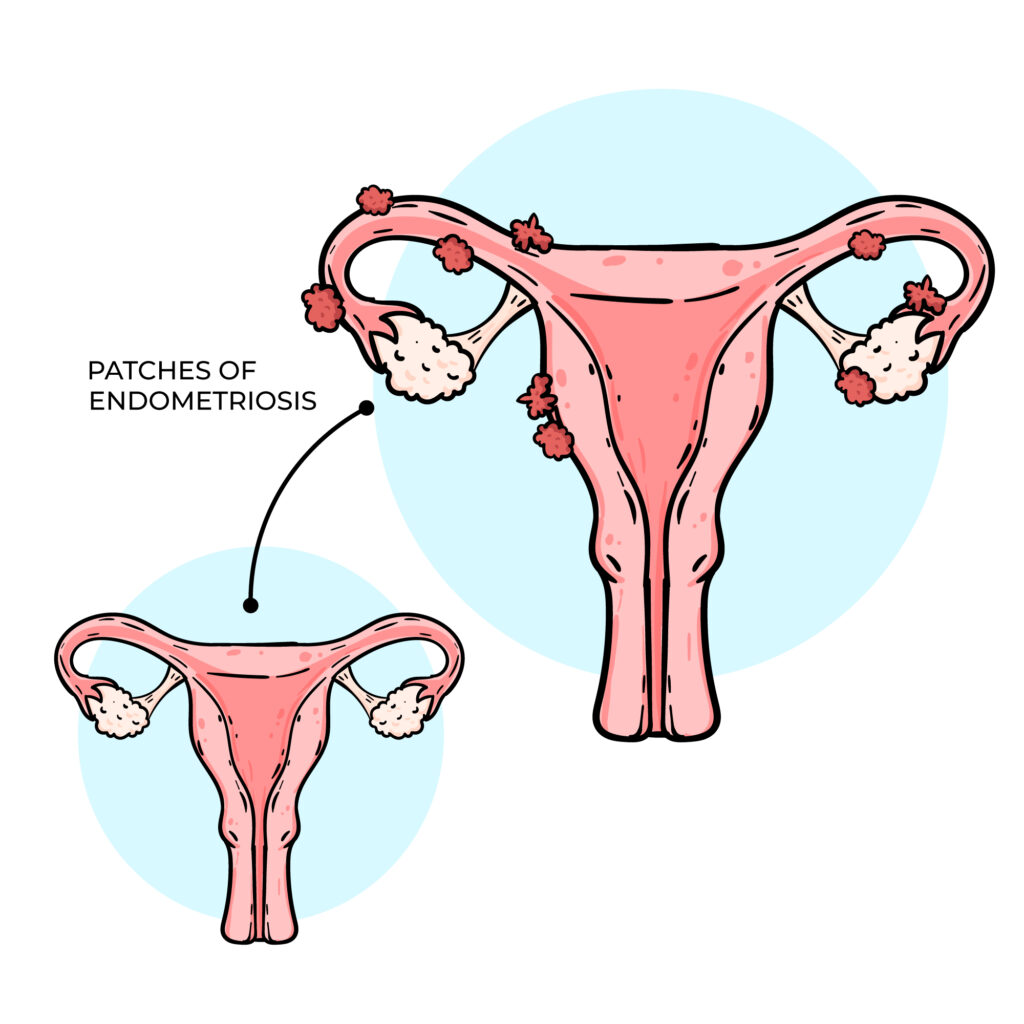
Endometriosis occurs when the tissue that normally lines the uterus and sheds during menstruation grows outside its usual place, often causing painful periods and affecting fertility. This tissue can grow within the womb’s lining and continue to spread as long as menstruation continues. Complete removal is usually not possible, as taking out too much can damage the uterus and affect the ability to carry a pregnancy, In severe cases, surgery may be done to remove some of the tissue, followed by hormone injections that stop menstruation for 3-6 months, allowing remaining tissue to shrink. However, a more effective approach may be to register with an IVF clinic, undergo endometriosis surgery, and then begin IVF treatment while menstruation is suppressed. This gives the body a better chance to conceive while preventing further tissue growth. It’s important to check and balance your AMH levels and hormones before surgery to improve your chances of success.
WHEN YOUR AMH VALUE IS ABOVE 3.5NG/ML AND YOU DON’T HAVE SIGNS AND SYMPTOM OF PCOS.
Anti-Müllerian Hormone (AMH) is a crucial marker used to assess a woman’s ovarian reserve in fertility evaluations. The typical reference range for AMH is approximately 1.0 to 3.5 ng/mL. Values below 1.0 ng/mL may indicate diminished ovarian reserve, while levels above 3.5 ng/mL can be suggestive of Polycystic Ovary Syndrome (PCOS). However, it’s important to note that not all women with elevated AMH levels present with the classical symptoms of PCOS, such as irregular menstrual cycles, acne, or anovulation. This condition is often referred to as “subclinical” or “silent PCOS”, where hormonal imbalance exists without obvious external signs. A high AMH level without symptoms may still affect egg quality and fertilization potential, potentially impacting conception outcomes. It is essential not to rely solely on regular menstruation or ovulation as indicators of reproductive health. If your AMH is above 3.5 ng/mL, or falls below 1.0 ng/mL, it is advisable to consult a fertility specialist for comprehensive evaluation and guidance on appropriate treatment or management strategies.
DIFFERENT TYPES OF FALLOPIAN TUBES DAMAGE.
Fallopian tube damage is a significant factor in female infertility. Common types of tubal pathology include: 1. Tubal Blockage: Where the fallopian tube is not patent (i.e., not open), preventing the passage of sperm or egg. 2. Hydrosalpinx: A condition where the tube becomes swollen and fluid-filled due to chronic inflammation, often impairing fertility. 3. Fimbrial Adhesions: Adhesions or scarring at the fimbrial end of the tube (the finger-like projections that help capture the egg from the ovary), which can block egg pick-up and transport. If one fallopian tube is damaged or surgically removed commonly after an ectopic pregnancy the other may still function and allow for natural conception. However, if one tube has hydrosalpinx, the toxic fluid it contains may backflow into the uterus and impair implantation, thereby affecting both natural and assisted conception (including IVF). A potential intervention is hydrotubation or tubal flushing, which aims to restore tubal patency. However, this procedure carries no guarantee of success and outcomes remain uncertain. After three months of any tubal treatment, a follow-up Hysterosalpingography (HSG) is recommended to reassess tubal status. If the tubes remain blocked or hydrosalpinx persists, in vitro fertilization (IVF) may be the most appropriate option for achieving pregnancy.
WHEN THERE IS NO GOOD RESULT FROM THE TREATMENT OF SEMEN PROBLEM.
There are instances where men undergo treatment for abnormal semen parameters, yet see little or no improvement in their semen analysis. For example, the sperm count may remain persistently low between 2 million and 10 million per milliliter or may even decline further, despite ongoing medication or therapy. In some cases, hormonal profiles and scrotal ultrasound results appear normal, yet sperm count, motility, and morphology fail to improve. One often overlooked cause is a blockage or dysfunction in the epididymis the coiled tube located at the back of the testicle where sperm is stored and matures. If this duct is obstructed or not functioning properly, sperm cannot pass through effectively, and medical treatments aimed at boosting sperm production may not yield results. In such cases, it is essential to consult a qualified fertility specialist or andrologist who can identify the underlying issue and recommend appropriate management options, which may include further diagnostic evaluation, surgical intervention, or assisted reproductive techniques such as IVF with ICSI.
SEVERE LOW SPERM COUNT AND AZOOSPERMIA
If you have been diagnosed with azoospermia (complete absence of sperm in the ejaculate) or severe oligospermia (sperm count less than 5 million/ml), it’s important to understand that the chances of spontaneous recovery with medication alone are often limited. Be cautious of anyone claiming to have a guaranteed cure. There are two main types of azoospermia: 1. Obstructive Azoospermia This occurs when sperm production in the testicles is normal, but a blockage prevents the sperm from reaching the ejaculate. Common causes include obstructions in the epididymis, vas deferens, or ejaculatory ducts, and may present as an epididymal cyst. These cases are often challenging and require evaluation by a urologist or male fertility specialist for possible surgical correction or assisted reproductive options like sperm retrieval. 2. Non-Obstructive Azoospermia This form results from impaired or absent sperm production by the testicles. In such cases, a scrotal ultrasound and hormonal profile (e.g., FSH, LH, testosterone) are essential to assess testicular function. Possible causes include undescended testes (cryptorchidism) or testicular failure due to heat damage or developmental issues. If the testes did not properly descend during childhood and remained inside the body beyond puberty, heat exposure may have irreversibly damaged sperm-producing cells. A quick self-check: normally, both testicles should be present in the scrotal sac, located below the penis. During cold temperatures, the scrotum may contract, but the testes should not retract entirely into the body. If you suspect you have a sperm production issue or have been diagnosed with azoospermia or severe oligospermia, consult a fertility scientist.